Articles
- Page Path
- HOME > Acute Crit Care > Volume 34(4); 2019 > Article
-
Original Article
Rapid response system Effect of a rapid response system on code rates and in-hospital mortality in medical wards -
Hong Yeul Lee1
 , Jinwoo Lee1, Sang-Min Lee1, Sulhee Kim2, Eunjin Yang2, Hyun Joo Lee3, Hannah Lee4, Ho Geol Ryu4, Seung-Young Oh5,6, Eun Jin Ha6, Sang-Bae Ko7, Jaeyoung Cho1
, Jinwoo Lee1, Sang-Min Lee1, Sulhee Kim2, Eunjin Yang2, Hyun Joo Lee3, Hannah Lee4, Ho Geol Ryu4, Seung-Young Oh5,6, Eun Jin Ha6, Sang-Bae Ko7, Jaeyoung Cho1 -
Acute and Critical Care 2019;34(4):246-254.
DOI: https://doi.org/10.4266/acc.2019.00668
Published online: November 29, 2019
1Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea
2Rapid Response Team, Seoul National University Hospital, Seoul, Korea
3Department of Thoracic and Cardiovascular Surgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul
4Department of Anesthesiology and Pain Medicine, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea
5Department of General Surgery, Seoul National University Hospital, Seoul, Korea
6Critical Care Center, Seoul National University Hospital, Seoul, Korea
7Department of Neurology, Seoul National University Hospital, Seoul, Korea
- Corresponding author Jaeyoung Cho Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul National University Hospital, 101 Daehak-ro, Jongno-gu, Seoul 03080, Korea Tel: +82-2-2072-2503 Fax: +82-2-762-9662 E-mail: apricot6@snu.ac.kr
Copyright © 2019 The Korean Society of Critical Care Medicine
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Background
- To determine the effects of implementing a rapid response system (RRS) on code rates and in-hospital mortality in medical wards.
-
Methods
- This retrospective study included adult patients admitted to medical wards at Seoul National University Hospital between July 12, 2016 and March 12, 2018; the sample comprised 4,224 patients admitted 10 months before RRS implementation and 4,168 patients admitted 10 months following RRS implementation. Our RRS only worked during the daytime (7 AM to 7 PM) on weekdays. We compared code rates and in-hospital mortality rates between the preintervention and postintervention groups.
-
Results
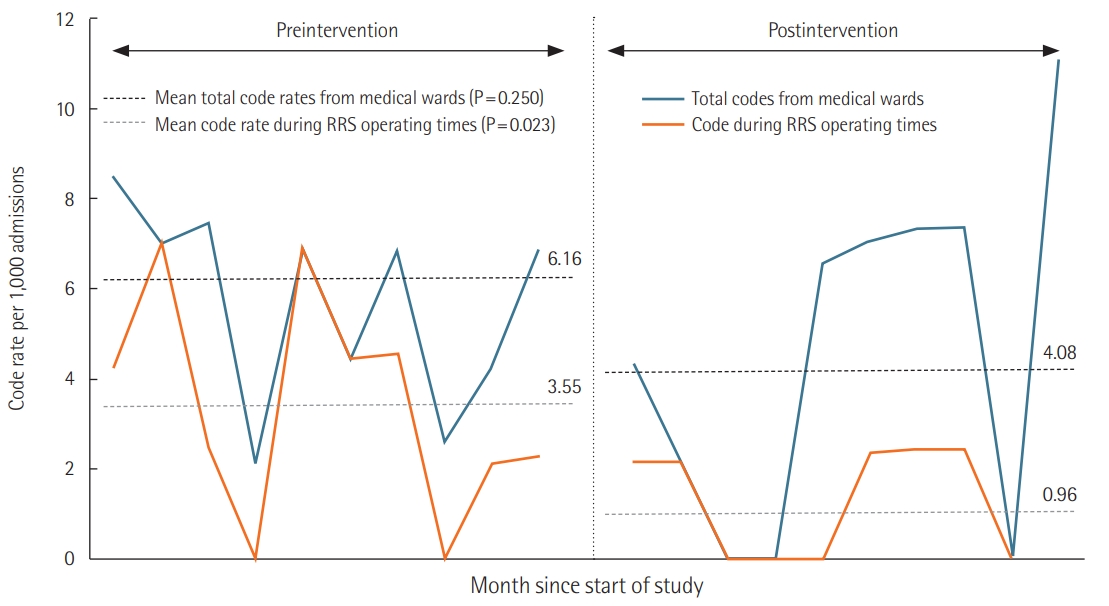
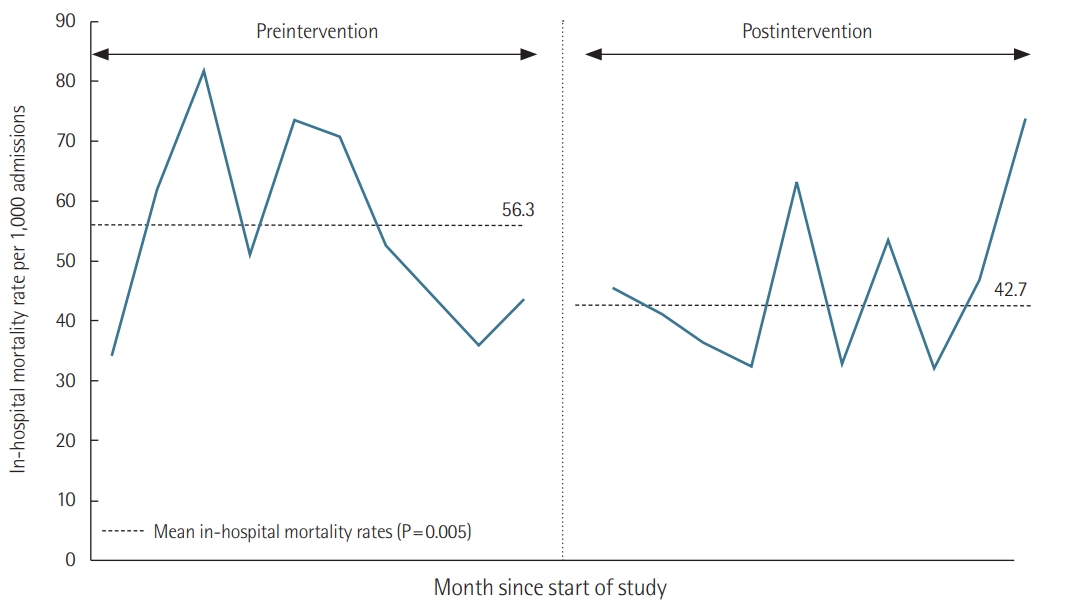
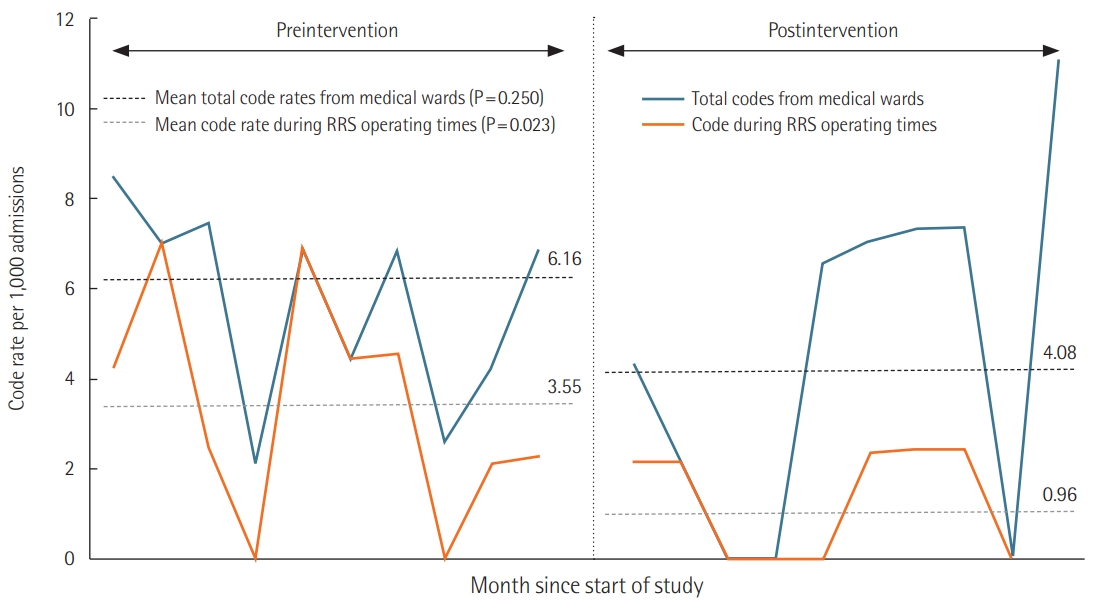
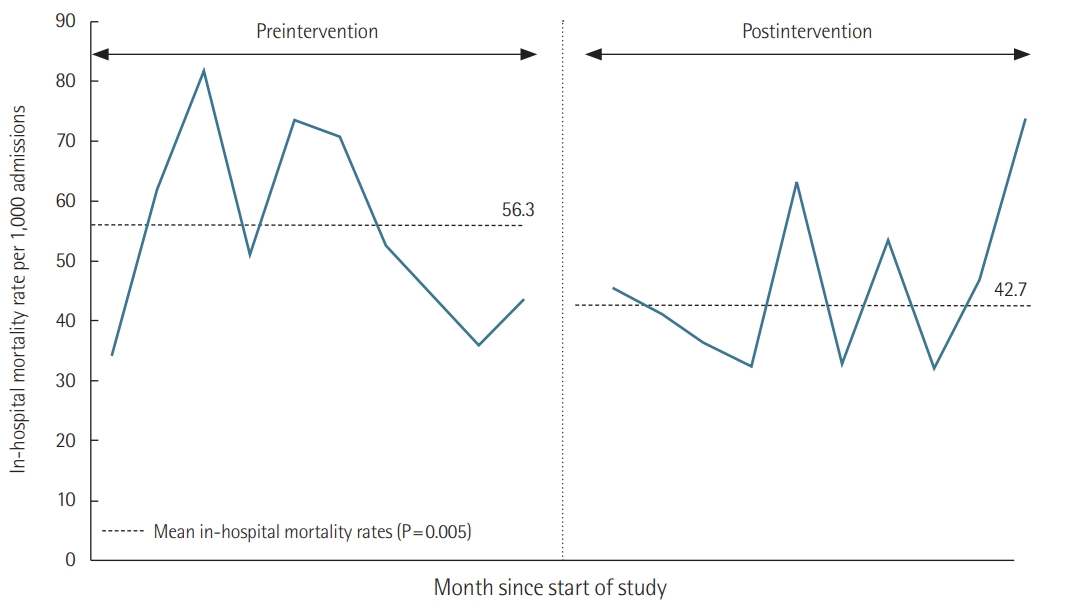
- There were 62.3 RRS activations per 1,000 admissions. The most common reasons for RRS activation were tachypnea or hypopnea (44%), hypoxia (31%), and tachycardia or bradycardia (21%). Code rates from medical wards during RRS operating times significantly decreased from 3.55 to 0.96 per 1,000 admissions (adjusted odds ratio [aOR], 0.29; 95% confidence interval [CI], 0.10 to 0.87; P=0.028) after RRS implementation. However, code rates from medical wards during RRS nonoperating times did not differ between the preintervention and postintervention groups (2.60 vs. 3.12 per 1,000 admissions; aOR, 1.23; 95% CI, 0.55 to 2.76; P=0.614). In-hospital mortality significantly decreased from 56.3 to 42.7 per 1,000 admissions after RRS implementation (aOR, 0.79; 95% CI, 0.64 to 0.97; P=0.024).
-
Conclusions
- Implementation of an RRS was associated with significant reductions in code rates during RRS operating times and in-hospital mortality in medical wards.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
DISCUSSION
HIGHLIGHTS
-
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conceptualization: JC. Data curation: EY, SK. Formal analysis: HYL. Methodology: HJL, HL, SYO, EJH. Project administration: SML, SBK, HGR. Visualization: HYL. Writing - original draft: HYL. Writing - review & editing: JC, SML, JL.
NOTES
| Variable | Preintervention (n=4,224) | Postintervention (n=4,168) | P-value |
|---|---|---|---|
| Age (yr) | 61.7±15.4 | 61.3±15.2 | 0.330 |
| Sex | 0.525 | ||
| Female | 1,778 (42.1) | 1,784 (42.8) | |
| Male | 2,446 (57.9) | 2,384 (57.2) | |
| Admitting specialty | <0.001 | ||
| Respiratory | 1,345 (31.8) | 1,396 (33.5) | |
| Hemato-oncology | 1,389 (32.9) | 1,220 (29.3) | |
| Gastroenterology | 709 (16.8) | 934 (22.4) | |
| Cardiology | 482 (11.4) | 369 (8.9) | |
| Nephrology | 79 (1.9) | 73 (1.8) | |
| Othersa | 220 (5.2) | 176 (4.2) | |
| Vital sign | |||
| Respiratory rate (/min) | 20 (20–20) | 20 (20–20) | 0.545 |
| Body temperature (°C) | 36.6 (36.3–36.9) | 36.5 (36.3–36.8) | 0.044 |
| Systolic blood pressure (mm Hg) | 123 (111–136) | 124 (112–136) | 0.065 |
| Diastolic blood pressure (mm Hg) | 75 (68–83) | 75 (68–83) | 0.180 |
| Heart rate (/min) | 83 (73–96) | 82 (71–94) | <0.001 |
| MEWS | 1.6±1.1 | 1.5±1.0 | <0.001 |
| MEWS critical score | 0.294 | ||
| <5 | 4,121 (97.6) | 4,058 (97.9) | |
| ≥5 | 102 (2.4) | 85 (2.1) |
| Variable | RRS activation (N=260) |
|---|---|
| Call of care from the RRS per 1,000 admissions | 62.3 |
| Male sex | 156 (60.0) |
| Age (yr) | 60.7±15.2 |
| Modified Early Warning Score | 4.7±2.1 |
| Medical specialty for admitted patients | |
| Hemato-oncology | 132 (50.8) |
| Respiratory | 105 (40.4) |
| Gastroenterology | 20 (7.7) |
| Cardiology | 2 (0.8) |
| Nephrology | 1 (0.4) |
| Endocrinology | 1 (0.4) |
| Route of RRS activation | |
| RRS member | 231 (88.8) |
| Nurse | 22 (8.5) |
| Physician | 7 (2.7) |
| Reason cited for activating RRSa | |
| Respiratory reason | 194 (74.6) |
| Respiratory rate ≤8 or ≥28/min, sudden stridor, or use of accessory muscles | 114 (43.8) |
| Oxygen saturation <90% | 80 (30.8) |
| Circulatory reason | 106 (40.8) |
| Heart rate ≤40 or ≥130/min, symptomatic arrhythmia | 54 (20.8) |
| Systolic blood pressure ≤80 or ≥200 mm Hg | 52 (20.0) |
| Staff worried: concern about overall deterioration | 23 (8.8) |
| Altered neurological status, seizure | 7 (2.7) |
| Body temperature >39°C or <36°C | 7 (2.7) |
| Laboratory reason | 10 (3.9) |
| Abnormal arterial blood gas test: pH <7.25, PaCO2 >50 mm Hg, or PaO2 <55 mm Hg | 5 (1.9) |
| Metabolic acidosis: lactic acid >4 mEq/L, total CO2 <15 mmol/L | 3 (1.2) |
| Electrolyte imbalance (potassium, magnesium, phosphate, calcium) | 2 (0.8) |
| Outcomea | |
| Consultation by RRS physician | 93 (35.7) |
| Transfer to ICU | 56 (21.5) |
| Intervention by RRS physician | 53 (20.4) |
| Intervention by RRS nurse | 45 (17.3) |
| Accompanying patient to radiology | 12 (4.6) |
| Transfer to operating room | 1 (0.4) |
| Outcome | Estimate (SE) | Adjusted ORa (95% CI) | P-value |
|---|---|---|---|
| Total codes from medical wards | –0.36 (0.31) | 0.70 (0.38–1.27) | 0.242 |
| Code from medical wards during RRS operating times | –1.24 (0.57) | 0.29 (0.10–0.87) | 0.028 |
| Code from medical wards during RRS nonoperating times | 0.21 (0.41) | 1.23 (0.55–2.76) | 0.614 |
| Code for the first 24 hours of unplanned ICU admission from medical wards | –0.97 (0.48) | 0.39 (0.15–0.99) | 0.047 |
| In-hospital mortality rate per 1,000 admissions | –0.24 (0.10) | 0.79 (0.64–0.97) | 0.024 |
Our RRS worked during daytime hours (7 AM to 7 PM) on weekdays.
RRS: rapid response system; SE: standard error; OR: odds ratio; CI: confidence interval; ICU: intensive care unit; MEWS: Modified Early Warning Score.
a Adjusted for age, sex, admitting specialty, and critical score of MEWS at admission.
- 1. Jones D, Rubulotta F, Welch J. Rapid response teams improve outcomes: yes. Intensive Care Med 2016;42:593-5.ArticlePubMedPDF
- 2. Litvak E, Pronovost PJ. Rethinking rapid response teams. JAMA 2010;304:1375-6.ArticlePubMed
- 3. Neumar RW, Shuster M, Callaway CW, Gent LM, Atkins DL, Bhanji F, et al. Part 1: executive summary: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015;132(18 Suppl 2):S315-67.ArticlePubMed
- 4. McGaughey J, Alderdice F, Fowler R, Kapila A, Mayhew A, Moutray M. Outreach and Early Warning Systems (EWS) for the prevention of intensive care admission and death of critically ill adult patients on general hospital wards. Cochrane Database Syst Rev 2007;(3):CD005529. ArticlePubMed
- 5. Chan PS, Jain R, Nallmothu BK, Berg RA, Sasson C. Rapid response teams: a systematic review and meta-analysis. Arch Intern Med 2010;170:18-26.ArticlePubMed
- 6. Salvatierra G, Bindler RC, Corbett C, Roll J, Daratha KB. Rapid response team implementation and in-hospital mortality. Crit Care Med 2014;42:2001-6.ArticlePubMed
- 7. Jung B, Daurat A, De Jong A, Chanques G, Mahul M, Monnin M, et al. Rapid response team and hospital mortality in hospitalized patients. Intensive Care Med 2016;42:494-504.ArticlePubMedPDF
- 8. Maharaj R, Raffaele I, Wendon J. Rapid response systems: a systematic review and meta-analysis. Crit Care 2015;19:254. ArticlePubMedPMCPDF
- 9. Solomon RS, Corwin GS, Barclay DC, Quddusi SF, Dannenberg MD. Effectiveness of rapid response teams on rates of inhospital cardiopulmonary arrest and mortality: a systematic review and meta-analysis. J Hosp Med 2016;11:438-45.ArticlePubMed
- 10. Lee BY, Hong SB. Rapid response systems in Korea. Acute Crit Care 2019;34:108-16.ArticlePubMedPMCPDF
- 11. Subbe CP, Kruger M, Rutherford P, Gemmel L. Validation of a modified Early Warning Score in medical admissions. QJM 2001;94:521-6.ArticlePubMedPDF
- 12. Hillman K, Chen J, Cretikos M, Bellomo R, Brown D, Doig G, et al. Introduction of the medical emergency team (MET) system: a cluster-randomised controlled trial. Lancet 2005;365:2091-7.ArticlePubMed
- 13. Jones DA, DeVita MA, Bellomo R. Rapid-response teams. N Engl J Med 2011;365:139-46.ArticlePubMed
- 14. Jones D, Bellomo R, DeVita MA. Effectiveness of the medical emergency team: the importance of dose. Crit Care 2009;13:313. ArticlePubMedPMC
- 15. Lee YJ, Park JJ, Yoon YE, Kim JW, Park JS, Kim T, et al. Successful Implementation of a Rapid Response System in the Department of Internal Medicine. Korean J Crit Care Med 2014;29:77-82.ArticlePDF
- 16. Lee YJ, Lee DS, Min H, Choi YY, Lee EY, Song I, et al. Differences in the clinical characteristics of rapid response system activation in patients admitted to medical or surgical services. J Korean Med Sci 2017;32:688-94.ArticlePubMedPMC
- 17. Tabak YP, Johannes RS, Silber JH, Kurtz SG. Should Do-NotResuscitate status be included as a mortality risk adjustor? The impact of DNR variations on performance reporting. Med Care 2005;43:658-66.ArticlePubMed
References
Figure & Data
References
Citations
- The role of emergency medical services in the management of in-hospital emergencies: Causes and outcomes of emergency calls – A descriptive retrospective register-based study
Henna Myrskykari, Timo Iirola, Hilla Nordquist
Australasian Emergency Care.2024; 27(1): 42. CrossRef - Effects of a Rapid Response Team on Patient Outcomes: A Systematic Review
Qiuxia Zhang, Khuan Lee, Zawiah Mansor, Iskasymar Ismail, Yi Guo, Qiao Xiao, Poh Ying Lim
Heart & Lung.2024; 63: 51. CrossRef - Society of Critical Care Medicine Guidelines on Recognizing and Responding to Clinical Deterioration Outside the ICU: 2023
Kimia Honarmand, Randy S. Wax, Daleen Penoyer, Geoffery Lighthall, Valerie Danesh, Bram Rochwerg, Michael L. Cheatham, Daniel P. Davis, Michael DeVita, James Downar, Dana Edelson, Alison Fox-Robichaud, Shigeki Fujitani, Raeann M. Fuller, Helen Haskell, Ma
Critical Care Medicine.2024; 52(2): 314. CrossRef - Improving sepsis recognition and management
Merrilee I Cox, Hillary Voss
Current Problems in Pediatric and Adolescent Health Care.2021; 51(4): 101001. CrossRef - A Somogy Megyei Kaposi Mór Oktató Kórház által bevezetett gyors reagálású rendszer hatása a kórházi mortalitásra
János Fogas, Rita Koroseczné Pavlin, Krisztina Szabó, Eszter Héra, Imre Repa, Mariann Moizs
Orvosi Hetilap.2021; 162(20): 782. CrossRef - Evidence revealed the effects of rapid response system
Jae Hwa Cho
Acute and Critical Care.2019; 34(4): 282. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite